
My attempt at trying to organize all the information I’ve come across in our healing.
Diagnosis
What is DID?
How does DID develop?
When faced with an overwhelming traumatic situation, a child may “go away” inside their head in order to escape. This is a normal coping mechanism for a child. Over time, as trauma continues, the dissociative escape is so effective that children may automatically use it whenever they feel threatened or anxious (even if the situation is not extreme or abusive). Repeated dissociation before the ages of 6-9 may result in a series of separate mental states, which may take on identities of their own to become a DID system.
What are the symptoms?
People with DID can experience hearing voices (within the mind), headaches, amnesia, time loss, trances, and “out of body” experiences. As a result of co-existing post traumatic stress, they may also experience any of the following:
- Depression
- Mood Swings
- Suicidal tendencies
- Sleep disorders (insomnia, night terrors, sleep walking)
- Substance Use Disorders
- Compulsions and rituals
- Psychotic-like symptoms (flashbacks in the form of auditory and visual hallucinations)
- Eating Disorders
Who gets DID?
Individuals who develop DID have experienced repetitive, overwhelming and often life-threatening trauma before the ages of 6-9 (a sensitive developmental stage of childhood). The most frequent type of trauma is extreme abuse, but survivors of other kinds of trauma (natural disasters, invasive medical procedures, war, kidnapping, and torture) have also reacted by developing Dissociative Disorders.
Can DID be cured?
Yes. DID is highly responsive to traditional talk therapy and it has a very good prognosis if proper treatment is applied.
How do I get diagnosed?
Description of the Process
Diagnosis is generally dependent on the DSM 5 (Diagnostic and Statistical Manual, fifth edition) which is published by the American Psychological Association (APA) and mainly used in the United States and Canada. In Europe, the ICD-10 (International Classification of Diseases, tenth edition) is more often used.
There is ongoing debate about diagnostic criteria for DID. There is criticism that the criteria is too abstract, making it difficult for the average clinician to assess. Some specialists have suggested that Dissociative Disorders should be re-classified to belong to a spectrum of Trauma Disorders.
A number of diagnostic tools may be used to assist with diagnosis. The “gold standard” is generally considered to be the SCID-D. It is a semi-structured clinical interview where the therapist asks open-ended questions and is trained to note subtle indicators of dissociation.
Who can diagnose DID?
The general answer is: any mental health clinician who is licensed to practice. This can include psychiatrists, licensed psychologists, and licensed clinical social workers.
However, many clinicians do not accept the existence of DID, having been taught incorrectly that it is rare or controversial. Clinicians who do believe in the validity of the diagnosis may have received little or no training in Dissociative Disorders or do not know how to recognize the symptoms.
It is imperative that the therapist is specialized in the treatment of DID, and that the client feels comfortable working with them. “Shop until you find the best fit” is a good saying to go by.
How do I find a therapist?
There are several places to contact if you are looking for clinicians who are trained in Dissociative Disorders.
- ISSTD Therapist Locator – This is the directory of clinicians who are members of the International Society for the Study of Trauma and Dissociation (ISSTD).
- Beauty After Bruises – A non-profit designed to support survivors of childhood trauma with CPTSD and/or Dissociative Disorders. They maintain a list of the psychiatric hospitals in the United States that have specialized programs for DID.
- PODS – Maintains a list of private individuals and organizations who provide diagnostic services in the UK.
What to Ask a Therapist
A therapist should understand and encourage your right to make an informed decision about your therapy. If the therapist seems offended or is unwilling to answer questions, take note of the red flag and move on. Here are some basic questions you may want to ask.
Do you treat DID? The most important issue in any DID treatment is empowering the client to live a more integrated life, with increased awareness and internal cooperation. This does not mean that parts have to disappear or cease to exist.
Are you licensed? A license means that a therapist has completed the requirements set by a licensing board in order to practice. It does not guarantee they are a good therapist, but it does mean they have had certain education and training. Likewise, an unlicensed therapist does not automatically mean the therapist is bad, but you may want to make sure they have the same training as their licensed counterparts. The most important thing is making sure the person has appropriate training in treatment of DID. If they do not have this training, they should at least have a supervisor who does.
Do you see fusion as a necessary goal of treatment? Fusion is two parts coming together to form a single state. The decision of fusion always lies with the client, not the therapist.
How do you deal with child parts? Pretending that parts do not exist is damaging, but any work done with parts should not create unnecessary dependency on the therapist.
How do you deal with angry parts? Angry parts are often protectors who keep the system safe by pushing outsiders away. The therapist needs to be comfortable with clients expressing anger and must also be able to establish clear boundaries.
DID vs. OSDD
DID/OSDD presentations
In Dissociative Identity Disorder (DID), a person does not have a unitary, single sense of self, but perceives themselves to be multiple. Different parts may become autonomous and identify themselves with different names. Parts may perceive themselves to be of different ages, genders, and will have in subtle or obvious ways very different ways of perceiving and relating to the world around them. Parts may shift, switch, or overlap in a number of ways.
When most people talk about Other Specified Dissociative Disorder (OSDD), they are referencing OSDD-1 (which stands for DSM subtype 1). This is used for individuals who appear very similar to DID but do not meet the full diagnostic criteria. The DSM divides OSDD-1 even further into subtype 1a and 1b.
OSDD-1a is DID with dissociated parts that are not fully evident, such as parts that do not switch forward, or parts that are less distinct.
OSDD-1b is DID with dissociated parts that do not experience the usual amnesia.
OSDD is often referred to as “not yet” or “not quite” DID. “Not yet” means the individual is perhaps new to therapy and based on their current internal awareness, they do not appear to meet the criteria for DID, but they will in the future. “Not quite” references people who have what appears to be DID but missing a feature, like amnesia. This has caused some professionals to support that OSDD and DID are the same thing, but at different points on a spectrum.
Polyfragmentation
Polyfragmented DID and OSDD systems simply involve a large number of parts. There is no specific number. Some professionals state polyfragmentation involves “dozens” of alters while others identify “over one hundred.” In a polyfragmented person, there is usually a smaller number of fully formed dissociated parts. The bulk of the parts are fragments, which are more one-dimensional. They may hold a single memory or feelings and never take over the body.
Dissociative Spectrum

Dissociation can be conceptualized as a continuum of severity, with “normal” everyday dissociative experiences occurring at the beginning of the continuum and Dissociative Trauma Disorders at the right of the continuum.
Treatment and Skills
All About Treatment
Phases
There are three common phases to trauma treatment.
- Safety and Stability
- Work on trauma memories
- Re-integration in to life
In DID-specific treatment, working directly with parts is critical to diminish symptoms and maximize resiliency. During Phase 1, individuals learn symptom management skills to help them manage symptoms of CPTSD and DID. A variety of therapeutic techniques may also help, along with medications to treat any co-occurring conditions.
Also critical in Phase 1 is negotiating safety with parts. Individuals may need to address suicidal or self-harming behaviors. Other potential areas to target are substance use disorders, eating disorders, high-risk behaviors, unsafe people, and other dangerous situations. This is because DID is developed in a childhood environment of repeated lack of safety and unpredictable danger.
Not all DID systems wish to address trauma in depth. However, for those that do wish to work on Phase 2, they will begin carefully and slowly exploring trauma memories. This is often experienced through flashbacks. Therefore, this phase involves ongoing safety and additional stabilization of DID and CPTSD symptoms.
In Phase 3, the individual’s DID and CPTSD symptoms have usually become much less intense. Parts do not disappear or go away. The goal of this phase is to be working cooperatively together, sharing information about switches when they do happen, so the individual can live and function without distress. Energy is directed towards living better in the present. Trauma is no longer the main focus. It becomes part of the person’s overall life story.
Inpatient
At times, a person with DID may struggle with symptoms such as intrusive thoughts, feelings related to traumatic events, emotional numbing, isolation, time loss, etc. to the extent that outpatient therapy is unable to progress. During these times, inpatient treatment with a DID program may help restore stabilization of symptoms and address any safety concerns.
See How Do I Find a Therapist? above for more information on locating a program.
Models and Approaches
Dialectical Behavioral Therapy (DBT) may help an individual build symptom management skills, particularly around distress tolerance, high-risk situations, unsafe people, and other dangerous situations.
Cognitive Behavioral Therapy (CBT) that is focused on trauma-related cognitive distortions can also be a helpful in phasic treatment.
Eye-Movement Desensitization and Reprocessing (EMDR) is a treatment that has been proven to reduce PTSD symptoms, particularly in people who have suffered adult trauma. EMDR, however, can significantly worsen the symptoms of DID, especially if used before the person is stabilized in treatment. EMDR can be an add-on treatment if the therapist has full training in EMDR and has specialized training in its use in DID.
Add On Treatments
Medications
There is no medication that treats DID symptoms. Usually, individuals with DID that take medications are treating other disorders or symptoms that are present. For example, a person with DID who has difficulty falling asleep, staying asleep, or with nightmares, may be prescribed a medication that specifically helps with PTSD nightmares. Nevertheless, the individual would still use symptom management skills to to assist with fears and flashbacks related to nighttime.
Group Therapy
A well-run group facilitated by a therapist with an established history of working with DID can be very helpful. A group can provide validation and support. It can be a venue to find encouragement, ask questions, seek our information, and request feedback. Although there are times it can be painfully hard to listen to others’ struggles, the group can be a place to work on staying present (and not dissociate) — both for the sharer and the listener.
Family Therapy
Involving a spouse, or significant other, can be important for many people with DID. In particular, family members may need education on complex trauma disorders and how to better support their loved one. Family or couples counseling may also be helpful to address healthy communication or problems in the relationship outside of DID.
Internal Communication
Getting to Know Your Parts
It is essential to get to know each individual part and the system as a whole. When beginning to build internal communication (or after having discovered a “new” part), it is important to create an environment where parts can feel safe and welcome. The system will need to:
- Get to know others inside
- Understand how life is now
- Understand how life is different from their past
Some systems find a journal or notebook a good solution.
Having a place where parts can write to one another facilitates internal communication and also allows the communication to go at a slow pace which may be easier to manage.
If a system is just starting out getting to know each other, it may help to break the process down. Give each part a page in a journal, or an index card, or a piece of construction paper for which they can choose a color, and invite them to write some things about themselves. Some basic ideas are: name, age (or age range), likes, and things that make them feel safe.
Some parts don’t have a name, or don’t like the name that was given to them. It’s perfectly ok to choose a name or change a name if the one given is too upsetting.
Young parts may want to tell their information to an older part who can write it down for them. Or, they may prefer to draw or collage.
A System Map is a common project therapists assign to expand on journal pages/index cards and get to know the system even better.
These can be done in many different formats, depending on what is easiest for the system to understand. It is not uncommon for systems to revisit mapping their parts as they become more aware of parts over time. Some examples of system maps are:
This is a challenging activity for many systems, since DID systems are geared to hide information. Parts may not want to participate. It can become frustrating and overwhelming trying to share information. Systems may also be fluid, with parts appearing, disappearing, or merging, when the system is under high stress. And for some systems, they simply may not find it helpful to create a System Map. That is okay, too, so remember to utilize what internal communication strategies work for your system.
Having an internal safe place is very important for DID systems.
Many people with a history of early trauma do not grow up in a safe environment where they developed nurturing relationships. As a result, an adult survivor lacks an inner sense of safety. They may not feel safe with their own inner experiences, such as their own emotions, thoughts, sensations, or parts. Parts may also be stuck in the past, during the trauma, and may not understand that their current environment is actually safe. Even the concept of safety can seem too foreign to survivors, or they may feel it is useless to try to think of a “calm place” because it’s so unknown.
For those who may be having trouble identifying safe places, here are some potential examples:
(1) Start small. Create a meeting room for parts to meet inside with one another.
(2) Pleasant outdoor places may include meadows, streams, or mountains.
(3) Some systems like to make safe homes such as cottages, beach houses, or tree houses.
(4) If you are having trouble coming up with items to include that feel safe, try The Store exercise (pg. 171-172, Coping With Trauma Related Dissociation). Here is a brief excerpt from the exercise:
Imagine a store in which anything you want or need as a resource for healing can be found and taken for free. This is no ordinary store, with ordinary aisles and ordinary merchandise. This is a magical place, a special place, beautiful and comfortable. Perhaps you see it as a quaint village shop, or an old bookstore with comfortable chairs and steaming pots of tea, or a sleek high-tech store with all the latest gadgets, where espresso and lattes are available as you browse. You can envision it in just the right way for you. It is your store that you create. In your shop you feel completely at ease, wandering up and down the familiar aisles, where the lighting and temperature are just right, where all is well and just as it should be. Perhaps it is quiet, or perhaps your favorite music is playing in the background. Perhaps there is even a little stage where your favorite musicians are performing just for you. This is one store wher eyou really enjoy lingering, choosing just the right items for your strength and protection. And indeed, there is an endless selection: shields; screens; transparents bubbles; magic stones; books of great wisdom; vials of liquid with healing properties; protective spirit or animal guides; magic cloaks of many colors, and some invisible to all but you; form-fitting lightweight suits of armor; emotional Kevlar, and on and on.Each is an equally strong and effective protection from the slings and arrows of life, from the vulnerability of being triggered. You may choose as many as you like, and exchange them as you wish. And as you wander around, or sit comfortably in a chair, allow all parts of you to have their time in this store, because it is for all of you.
One safe place may be sufficient for your system, but it’s also okay if parts feel the request different places that match their own needs.
Not all parts may want to participate and that’s fine. Just start where yous are able.
An internal meeting place is useful for parts when working on internal communication or trying to make decisions that require input from all parts.
Some systems hold daily meetings (at least once a day). They can be a time for parts to get to know each other. They can also be designated as check-ins to see how all parts are feeling. Some ideas for discussions include:
- Make sure the inner world (and/or meeting room) is safe.
- Talk about upcoming events or appointments.
- Any concerns, problems, or questions.
- Celebrate successes and good things going on.
The Internal Meeting Place worksheet can be helpful when developing a meeting room for the first time (or making updates).
Roles or Jobs
Sometimes parts are created, not because of trauma, but because of a stressful situation that was triggering. These parts may assume certain duties such as going to school, being a parent, handling social situations, going to work, or being intimate when in a marriage or committed relationship.
Some other commonly found parts include those who act as inner helpers, wise/knowledgeable ones, and protectors. Systems may call them by other names. Some systems may not have parts that have these functions at all.
Sometimes, protectors operate off of mistaken beliefs of what safety really is. These types of protectors may act inappropriately aggressive to drive others away. They may even bully or abuse other parts–sometimes to the point of self-harming the body. It is essential to work with a therapist regarding these parts so they can find healthier ways to continue to protect.
It is important that the system learns from one another, in order to eventually share responsibilities, tasks, and roles. This enables parts to take breaks from something hey have been doing for a very long time. Sharing is also a good idea in case the normal part that handles a task is not able or available.
Younger Parts
Younger parts often need the love and parenting the system did not receive as a child. Just like any child, they may need guidance and supervision to learn they can’t spend all the system’s money on video games or candy. And just like other parts, they may need to heal from the trauma.
Younger parts may need to learn not to “come out” at inappropriate times (such as at work, or when being intimate with a partner). Likewise, it is important that they have time in the outside world to fulfill their needs or wants. Some systems do this under pre-arranged times and agreed upon conditions.
Fear of Internal Communication
At times, a person with DID may have resistance to building internal communication, or they may feel overwhelmed when they attempt it. This is completely understandable, because information that a part holds can be emotionally charged, frightening, and uncomfortable.
It’s normal human instinct to want to avoid pain. People with DID and CPTSD get particularly skilled at avoidance through dissociation. An alternative today, instead, is using short-term avoidance such as distraction techniques, in order to “dial down” charged emotions so safety and stabilization skills may be used.
Tips & Tricks
Crisis Continuum
The Crisis Continuum is a detailed plan to help identify impulses on a continuum of severity. Then, for each level of severity, the individual identifies actions necessary to stay safe. This is a tool a DID person can use as part of Phase 1 Safety and Stabilization. See more about the Crisis Continuum here.
Containment
Containment is an essential strategy for managing DID and CPTSD. The use of the skill can help prevent an individual from becoming overwhelmed, help making safe choices, and increase the ability to tolerate strong feelings (anger, rage, sadness, terror, hopelessness, fear, anxiety).
Containment involves allowing feelings, thoughts, impulses, and images into your conscious awareness without being compelled to seek immediate understanding. Using specific techniques, they can be stored for retrieval at the appropriate time (such as during a therapy session), so they do not interfere with your ability to achieve your goals for the day. Containment allows you to explore, process, and deal with feelings, thoughts, images, and impulses safely.
Here are some great links from DID-SOS on containment:
Grounding
Grounding is a coping strategy to connect you to the present moment. Whereas dissociation is disconnection, grounding is connection. Grounding is usually the first new response we learn to have after being triggered, because if we aren’t present in our mind and body, then other coping skills will be unnecessarily hard to accomplish.
- Orientation Card – an index card you can tape to the front of your journal that explains how old the body is, where you live, who lives with you, and how the present is different from the past.
- 5 by 5 by 5 – Identify 5 things you see, 5 things you hear, and 5 things you can touch
- Identifying Anchors
- Take grounding walks (notice what you see, hear, etc.)
- Color Mandalas
- Drink ice water
- Hold a frozen orange (or lime if you are allergic to oranges)
- Do Level 1 journaling
- Play with a tangle or silly putty
- Make grounding beads
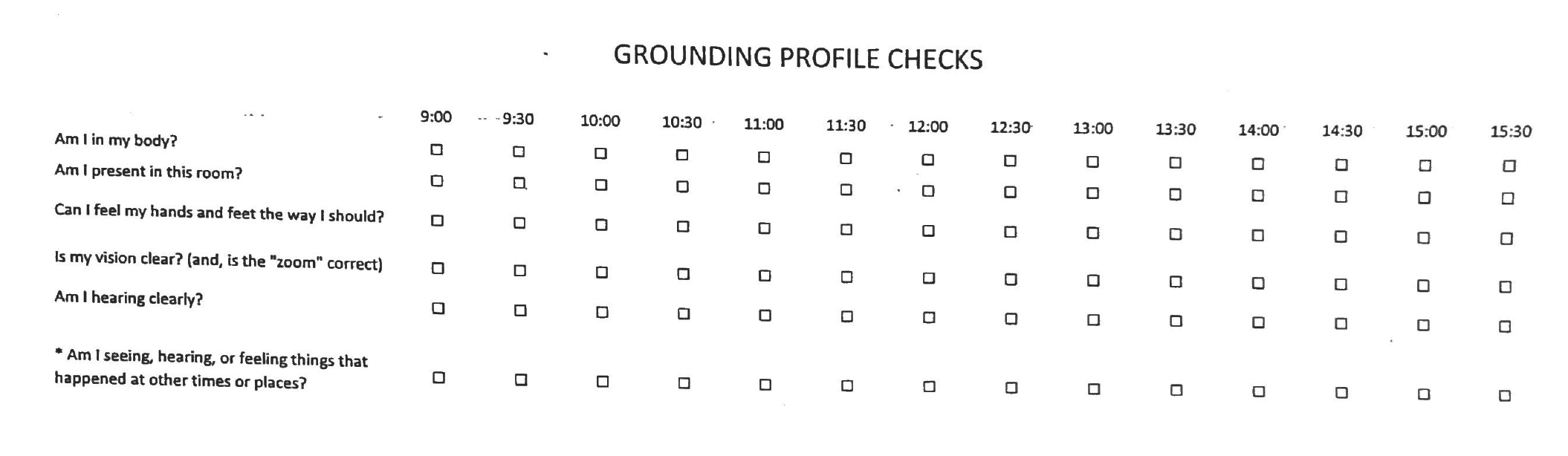
- Do grounding checks
- BONUS: Create a grounding bag or kit
Self-Soothing
These skills help an individual calm and relax when feeling overwhelmed. They are about being good and kind to yourself. These skills may also be called distress tolerance or emotion regulation. Some examples are:
- Light a scented candle, watch the flame, and enjoy the scent
- Listen to soothing music, or nature/ocean sounds
- Take a walk in a garden or the woods
- Cook a favorite meal
- Drink some hot cocoa, tea, or coffee
- Pet your dog or cat
- Take a bubble bath
- Practice deep breathing
- Chew gum
- Use a weighted blanket
Non-Verbal Expression
Sometimes called creative expression, these are “other than talking ” ways of telling a story, thoughts, or feelings. Creative expression is particularly helpful for people with DID. Trauma occurs at such a young age that the child may not have had a complete enough vocabulary to express what was happening to them. Thus, today as adults, people with DID continue to struggle finding the “right” words for something they never had words for. Creative expression can be things like:
- Make art with fingerpaints
- Experiment with a new kind of paint (oil, watercolor, pastel, charcoal, etc)
- Make a box you can use for Containment (collage/paint it with safe/soothing colors, images, etc)
- Color a suncatcher
- Make a scribble drawing
- Make a zentangle
Support
Outsiders
DID and Relationships
For someone with DID, all relationships can be challenging. Those with DID have the added task, constantly running in the background, of healing from traumas and improving internal relationships with parts. Choosing someone externally to share our lives with and let in on what has happened to us, in addition to the fact that we are a system, can be one of the greatest challengings of recovery.
The important precursor for many people with DID is accepting that we cannot expect a partner to save us. We must do the healing work to save our younger parts ourselves. We also cannot expect a partner to be the loving, nurturing parent our younger parts never had. We must be that parent to our inner children.
It is normal for a survivor to hope that someone will come along and rescue them. It is okay to talk about that desire and process it with a therapist or support person. A therapist should be able to guide and support an individual to find the tools to become a strong, independent person.
A common issue that comes up in intimate relationships is working with parts who may be triggered by sexual intimacy. This is where it is helpful to reflect back on inner safe places (above). A part who is triggered by this activity, or a younger part for whom it is inappropriate to engage in sexual activity, may wish to find a way of shielding themselves in the inner safe place during this time.
The system may also want to hold an internal meeting to discuss the relationship, and have agreed upon arrangements on who will engage in the activity. Some systems and their partner are comfortable with more than one part engaging in the activity, while other systems and their partner are not.
Parenting and DID
If you are, or suspect you may be, abusive to your children, get your children and yourself immediate professional help and intervention. In the United States, help for parents can be found by calling the National Parent Helpline at 1-855-427-2736. Help for child abuse victims and parents, call 1-800-4ACHILD.
In the beginning of therapy, or during stressful times of life, it may be helpful for the system to agree to only have certain parts forward dealing with outside children. Usually, there is at least one part that deals better with children and has more patience and parenting skills. Having parts like this agree to help can cut down on switching that may be confusing to some children.
At some point, parents may consider disclosing their DID diagnosis to their children. There is no right or wrong answer to this. It is a highly personal decision. Many systems consider what would be gained by telling or not telling. If it seems appropriate, disclosing DID in a healthy, gentle, and age-appropriate way will help the conversation. A helpful book may be My Mom Is Different which is a free book written for children.
DID and Work
Just like in other stressful areas, it may be helpful to designate a part (or parts) who handle going to work. Ideally, these parts would be the best skilled for the individual’s type of employment.
It may also be helpful to have a BDA Plan developed if the system expect a difficult time at work, such as a planned audit, important meeting with a client, etc.
Sometimes, while processing a particular difficult trauma, it may be difficult or impossible to work. We, personally, have had to reduce work hours or even take FMLA leave from work. We encourage systems to explore options as your system’s safety is always the #1 priority.
Coming Out DID
Disclosure of DID is a personal choice. There is no right or wrong. Here are some general points to keep in mind:
- Disclosure should be a system decision.
- Is this person loving, caring, supportive, and accepting of me in all areas of my life?
- Do I see or hear this person making offensive or disrespectful remarks about people with disabilities or mental health problems?
- What might the relationship gain or lose by disclosing our diagnosis?
- What is my reason for wanting to disclose to them?
- How will I tell this person about our parts? What exactly will I say? Will I explain how and why DID developed? Some people like to write this out in advance.
- How do I expect the person to react? How will we handle it if we receive a negative or hurtful response?
Telling Your Doctor
Even mental health professionals do not always understand DID, so it can be daunting to consider telling your doctor, or similar physician such as a dentist. If you find it is important to inform your doctor, you may consider writing them a letter, email, or having a conversation with them.
It may be helpful to explain that you think all medical providers should know about you and your background. These things are hard to say, but it is important to make sure you get the best healthcare possible.
You may wish to explain that you are a survivor of long-term abuse, but to clarify that you are in a safe situation today. You may also want to share that you are in therapy, including the name and contact information of your therapist. If you decide to specifically share your diagnosis, spell out the name of the disorder and be clear that it is a result of of the trauma and abuse.
You may also want to include anything that your parts would find helpful. For example, many child parts need to have things explained ahead of time, including when there will be a touch or whatever is involved in a procedure. This lessens anxiety and stress.
Your therapist may also be willing to talk to your doctor to explain any other questions the doctor or dentist may have.
Support Groups
Caution About Online Support
For many years, the professional DID experts have agreed that self-help or peer support groups should be discouraged for those with DID. The primary reason for this is not because therapists want to isolate trauma survivors from one another. The reason is because typically these groups are unformatted, and can result in emotional flooding or psychological distress.
However, there has been a peer support movement in the survivor community. Peers focus on what they can do for each other, and how they can help one another on a day-to-day basis. This is part of a n overall shift away from the medical model of treatment to a trauma model.
Many professionals are recognizing the benefits of these groups. With peer support, there is potential for people with DID to find a reduced sense of isolation when they realize they are not alone. Many others share similar symptoms and difficulties. Accountability also is a benefit of peer support. People with DID learn to take responsibility for their behavior, and hold members of the community responsible for their actions through feedback.
For those who decide to engage in peer support, members need to have good boundaries because the feelings associated with trauma can be very powerful at times. Remember, if you feel unsure of a particular group, it’s best to be cautious. Peer support groups must be safe.
Meetings & Groups
All groups have their pros and cons. People also have their own preferences for different platforms and group attitudes. For those reasons, I do not personally endorse one group over another. I encourage people to try different groups until they find the best fit for them.
This is not an exhaustive list of support groups, and we also encourage you to do your own research.
- Sidran Institute Help Desk – Can help you locate support groups for people who have suffered trauma.
- Anxiety and Depression Association of America – Offers a list of support groups, including PTSD.
- Survivors of Incest Anonymous (SIA) – A 12-step program for all survivors of childhood sexual abuse. The Coming Home Phone Line offers phone meetings daily, and there are even some for those who identify as multiple.
- Gift From Within – Global List of Trauma Support Groups (includes some for DID).
- Gift From Within – Offers a pen pal service for women. Email Joyce Boaz (Executive Director) at JoyceB3955@aol.com for more information.
- PTSD Peer Support for Police Officers
- Discussing Dissociation Community Forum
- Dissociative Identity Disorder Support on Reddit
- Mosaic Minds
- Support Groups in the UK
Resources
Books
TraumaDissociation.com has a concise list with descriptions of books here. Some of my personal favorites are:
- Coping With Trauma Related Dissociation – A great collection of information, exercises, and worksheets on dissociation symptom management.
- Dear Little Ones – A book written for child parts. You can watch a reading of the book on YouTube.
- Growing Beyond Survival: A Self-Help Toolkit for Managing Traumatic Stress – This book was developed with input from survivor advocates and field tested at Sheppard Pratt Trauma Disorders Unit.
- Managing Traumatic Stress Through Art – An art workbook developed by the co-founder of The Center at PIW.
Websites
- An Infinite Mind
- Beauty After Bruises
- DID-Research.org
- The CTAD Clinic YouTube Channel
- FirstPersonPlural.org.uk
- The Flock
- International Society for the Study of Trauma and Dissociation (ISSTD)
- Many Voices

{kind=link}